
What is AIM?
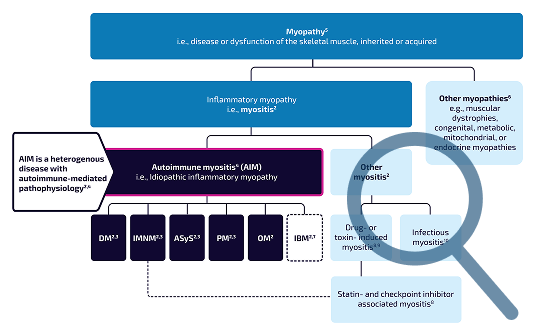
AIM is a rare autoimmune rheumatic disease spectrum, encompassing heterogeneous subtypes with diverse clinical presentations.3,4
A typical feature is progressive, symmetrical weakness of the proximal muscles. As a chronic, progressive condition with both muscular and extramuscular involvement, AIM can lead to loss of independence and a substantial impact on quality of life.2,5
AIM is comprised of subtypes with diverse manifestations and clinical concerns2,3
Muscle weakness is usually the common clinical manifestation, but other organs are often affected to varying degrees across subtypes.2,3

Dermatomyositis (DM)

Antisynthetase syndrome (ASyS)

Immune-mediated necrotizing myopathy (IMNM)

Polymyositis (PM)

Overlap myositis (OM)

Inclusion body myositis (IBM)

CLINICAL MAINFESTATIONS
How AIM presents and progresses
AIM comprises a spectrum of distinct subtypes with diverse clinical manifestations. While skeletal muscle weakness is the hallmark, the disease can also affect the skin, lungs, gastrointestinal tract, joints, and heart. Key complications of concern include associated malignancy, interstitial lung disease, skin involvement, myocarditis, and dysphagia.1,3
Continue exploring AIM
Learn more about the role of autoantibodies, the burden of disease, and current and emerging treatments.
Role of autoantibodies
Autoantibodies are a hallmark feature of AIM.6
Burden of disease
AIM can reshape the lives of patients and those around them.5
Current treatments
There remains an unmet need for effective and well-tolerated treatments for AIM.7
Abbreviations:
ADM, amyopathic dermatomyositis; AIM, autoimmune myositis; ASyS, antisynthetase syndrome; DM, dermatomyositis; HMGCR, 3-hydroxy-3-methylglutaryl-coenzyme A reductase; IBM, inclusion body myositis; IIM, idiopathic inflammatory myopathy; ILD, interstitial lung disease; IMNM, immune-mediated necrotizing myopathy; OM, overlap myositis; PM, polymyositis.
References:
1. Diomedi M, et al. Clin Exp Rheumatol. 2026;44(2):167–177; 2. Oldroyd A, et al. Clin Med (Lond). 2017;17(4):322–328; 3. Paik J, et al. Rheumatol. 2025;64:3288–3302; 4. Giannini M ,et al. Clin Exp Rheumatol. 2025;43:178–183; 5. Oldroyd A, et al. BMC Rheumatol. 2020;4:47; 6. Groener M, et al. Front Immunol. 2025;16:1581323; 7. Natour A and Kivity S. Rambam Maimonides Med J. 2023;14(2):e0008.