
Defining MSAs and MAAs1
Autoantibodies identified in AIM are broadly categorised as either myositis-specific autoantibodies (MSAs) or myositis-associated autoantibodies (MAAs).2,3
MSAs are considered relatively specific to AIM and are frequently associated with defined phenotypes.4 In contrast, MAAs may occur in AIM alongside other connective tissue diseases and overlap syndromes.2,4
Most patients with AIM have a single dominant MSA, which may correlate with characteristic patterns of muscle and extramuscular involvement.2,6

MSAs and clinical phenotype
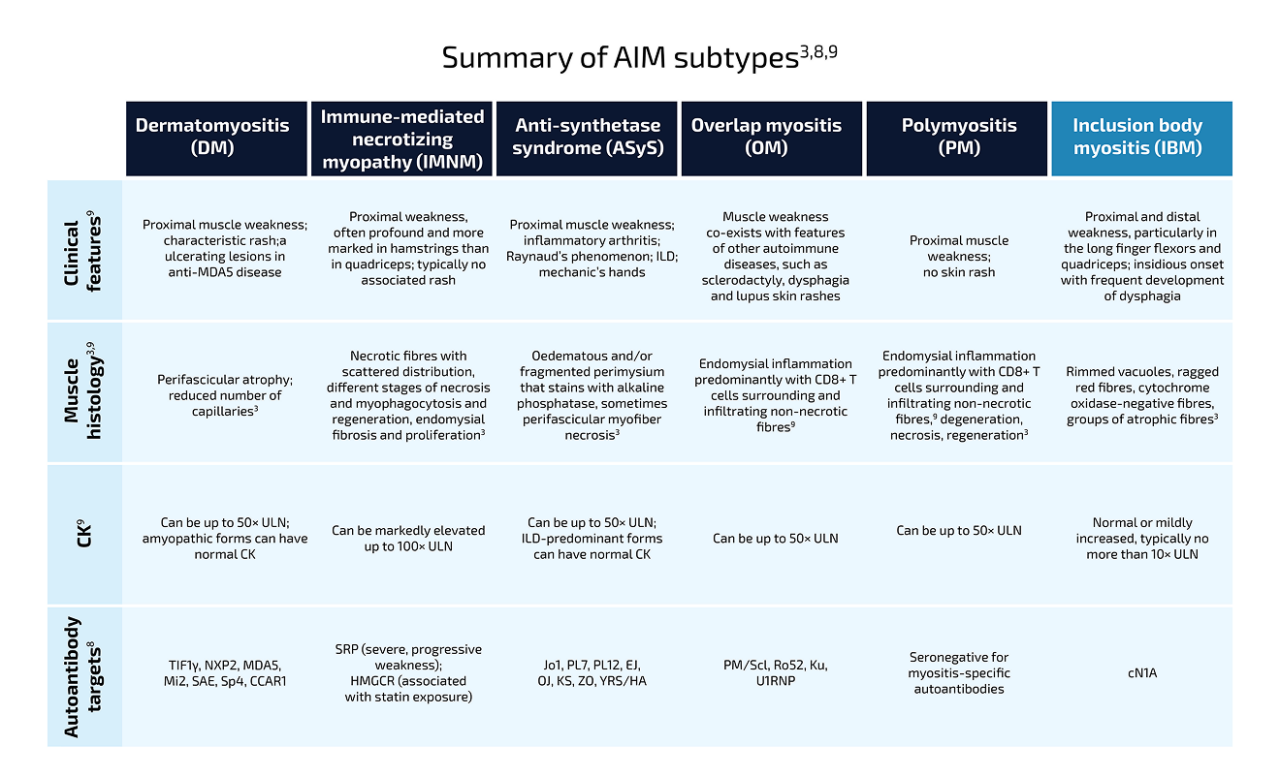
Distinct MSAs are associated with specific clinical manifestations, patterns of organ involvement, and disease trajectories.2,6–8
These associations have contributed to increasing recognition of AIM as a spectrum of autoantibody-defined disease subsets rather than a single clinical entity.2,6,8
Autoantibodies contribute to distinct muscle and organ
manifestations:5,10–12

Direct muscle injury
e.g., Anti-HMGCR, Anti-SRP5

Lung endothelial activation
e.g., Anti-Jo-15

Ulcerative/ vasculopathic skin lesions
e.g., Anti-MDA55

Dysphagia/GI involvement
e.g., Anti-FHL15

Cardiac involvement
e.g., Anti-SRP11
Subclinical organ involvement may occur even without overt symptoms: muscle involvement may be asymptomatic, and cardiac involvement in AIM is usually subclinical, with reported prevalence ranging from 4% to 26%; these may be difficult to detect without targeted assessment.12,13
Continue exploring AIM
Learn more about the role of autoantibodies in AIM
How AABs drive disease
Growing evidence suggests that autoantibodies contribute directly AIM pathogenesis.4
Diagnosis of AIM
Autoantibody testing has become an increasingly important component of diagnostic evaluation and subtype classification.2,4
Abbreviations:
AAB, autoantibody; ADM, amyopathic dermatomyositis; AIM, autoimmune myositis; CCAR-1, cell cycle and apoptosis regulator 1; CN1a, cytosolic 5’-nucleotodase 1A; EJ, glycyl-tRNA synthetase; FHL1, four-and-a-half LIM domain protein 1; GI, gastrointestinal; HMGCR, 3-hydroxy-3-methylglutaryl-CoA reductase; ILD, interstitial lung disease; KS, asparaginyl-tRNA synthetase; MAA, myositis-associated autoantibody; MDA5, melanoma differentiation-associated gene 5; MSA, myositis-associated autoantibody; NXP2, nuclear matrix protein 2; OJ, isoleucyl-tRNA synthetase; PL7, threonyl-tRNA-synthetase; PL12, alanyl-tRNA synthetase; PM/Scl, polymyositis–scleroderma overlap; SAE, small ubiquitin-like modified activating enzyme; Sp4, transcription factor Sp4; SRP, signal recognition particle; TIF1γ, transcription intermediary factor 1-gamma; U1RNP, U1 small nuclear ribonucleoprotein; ZO, phenylalanyl-tRNA synthetase.
References:
1. Groener M and Paik J. Front Immunol. 2025;16:1581323; 2. Wang G and McHugh NJ. Clin Exp Rheumatol. 2025;43(2):364–71; 3. Lundberg IE, et al. Nat Rev Dis Primers. 2021;7(1):87; 4. Halilu F, Christopher-Stine L. Rheumatol Immunol Res. 2022;3(1):1–10; 5. Wu Y, et al. Front Immunol. 2024;15:1439807; 6. Harvey GR, et al. Curr Rheumatol Rep. 2024;27(1):5; 7. Saygin D, et al. Rheum Dis Clin Rheum North Am. 2025;51(4):563–576; 8. Paik JJ, et al. Rheumatology (Oxford). 2025;64(6):3288–302; 9. Khoo T, et al. Nat Rev Rheumatol. 2023;19(11):695–712; 10. Diomedi M, et al. Clin Exp Rheumatol. 2026;44(2):167–177; 11. Bandeira M, et al. Front Immunol. 2023;14:1146817; 12. Zhu H, et al. J Inflamm Res. 2025;18:3879–3888; 13. Matsuda N, et al. Acta Radiol Open. 2022;11(2):20584601221075796.